Meniscal transplantation is a fairly major complex procedure. The surgery is not ‘big’ in terms of the size of the incisions, but the surgery is quite long (about 2 hours for an isolated meniscal transplant, longer if other concomitant procedures are undertaken at the same time) and it is a highly technically demanding.
There is only a small handful of surgeons in the UK who have undertaken any significant number of meniscal transplants and who have proper experience in this procedure.
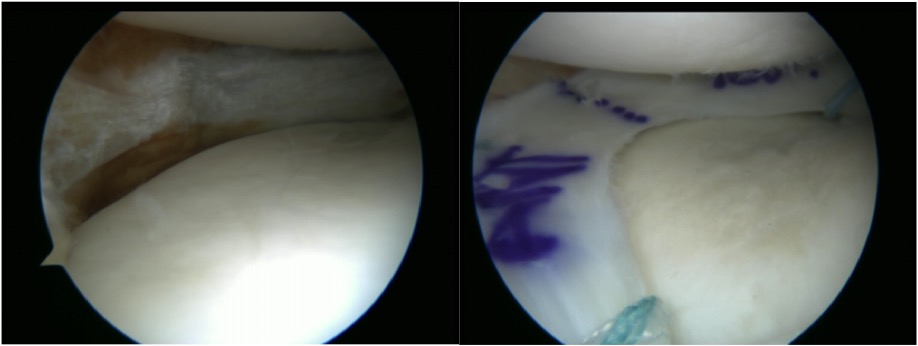
There are a variety of different surgical techniques that are used for meniscal transplantation, ranging from wide open surgery to keyhole, and from the use of large bone blocks to soft tissue fixation only. The technique that is favoured by most expert meniscal transplant surgeons involves minimally invasive keyhole surgery with fixation of the allograft to the bone of the tibia by transosseous sutures, as follows: